

CCTA and Calcium Score — two complementary exams
Although often performed in the same session, CCTA and CACS are two distinct exams. The Calcium Score (CACS) allows assessment of the calcium burden in the coronary arteries (an indirect measure of atherosclerosis), without contrast, with the images synchronised to the heartbeat through ECG electrodes. Cardiac CT angiography (CCTA) allows assessment of the anatomy of the coronary arteries (narrowings), with iodinated contrast and the same cardiac gating.
When it is requested
- Stable chest pain at low-to-moderate pre-test probability (5–50%). CCTA is first-line (ESC 2024 Class IA; AHA/ACC 2021 Class IA).
- Risk stratification in asymptomatic people: CACS is recommended by ACC/AHA 2019 (Class IIa) to inform the decision to start a statin at intermediate risk.
- Specific anatomical assessment: before non-cardiac surgery, congenital anomalies, follow-up of coronary bypass grafts or stents.
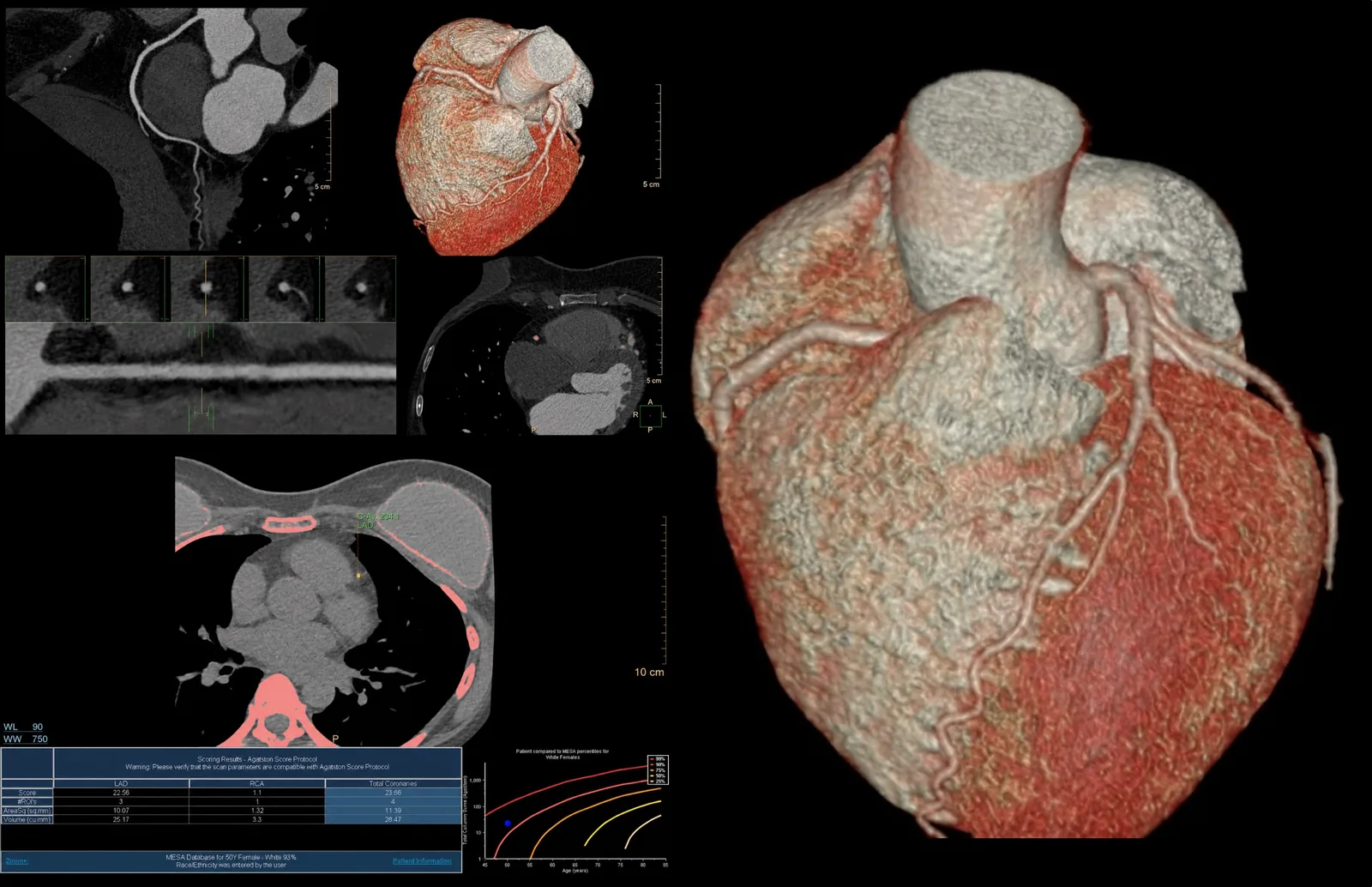
How the Calcium Score is interpreted
Clinically relevant categories (Agatston Score): 0 — no detectable calcium; 1–100 — mild calcium; 101–399 — moderate calcium; ≥400 — extensive calcium. The specific interpretation always rests with the doctor following your case — together with age, sex and risk factors.
What the exam is like
The exam in the room takes 15 to 30 minutes. Image acquisition takes seconds.
- 160 min before
Reception and cardiac preparation
Arrive 60 minutes before your appointment, for the cardiac preparation. Your heart rate is measured at reception. The exam takes place with a cardiologist present.
- 2
Heart-rate control
Target heart rate <60 bpm (up to 65 is acceptable). Depending on your rate, you may be given oral medication to lower it, 30 minutes to 1 hour before acquisition, according to CRMA's protocol. In particular cases the intravenous route is used — always by medical decision, with a cardiologist present and monitoring.
- 32–5 min before
Sublingual nitroglycerin
Given 2 to 5 minutes before acquisition, depending on your blood pressure. It may cause a passing headache (15–30 min).
- 4
ECG electrodes
3 or 5 ECG electrodes on the chest for cardiac gating.
- 5
Cannula in the arm
An 18G cannula, for the high flow rate of contrast.
- 65–10 s
Acquisition with a breath-hold
A breath-hold of 5–10 seconds during acquisition — the radiographer explains and practises it with you first.
Preparation — key points
- Arrival: 60 minutes before your appointment.
- In the 12–24 hours before: avoid coffee, black and green tea, caffeinated soft drinks, energy drinks, chocolate, tobacco/nicotine and other stimulants — they speed up the heart and make heart-rate control harder.
- 48–72 hours before: stop Sildenafil (Viagra), Tadalafil (Cialis), Vardenafil (Levitra). An absolute contraindication with the sublingual nitroglycerin used in the exam — risk of severe hypotension.
- Regular medication: keep it — including beta-blockers — unless your doctor advises otherwise. If needed, additional medication is given at the clinic, before the exam, according to CRMA's protocol. Let us know if you take medication for diabetes or anticoagulants.
- Keep your other cardiac medication: antihypertensives, antiplatelets, statins.
- Fasting: 4 hours.
- Kidney function: bring recent creatinine/kidney function blood tests (eGFR) — usually from the last 30 to 90 days, according to clinical risk. Let us know if you have kidney impairment or if you have had a reaction to iodinated contrast.
- Breastfeeding: always let us know. Breastfeeding may continue as normal after the contrast is given (ACR/ESUR recommendation).
- A recent ECG (if available) and a current list of your medication.
Results
The report follows the CAD-RADS classification (Coronary Artery Disease — Reporting and Data System), on a scale of 0 to 5. For findings suggestive of significant coronary artery disease (CAD-RADS 4–5), the radiologist ensures priority communication to the referring doctor.